From "Seinfeld": A bubble boy? | Yes, a bubble boy! | What's a bubble boy? | He lives in a bubble!
Narrator: For decades, his story has echoed through the popular culture.
From "Bubble Boy": Why are you in that bubble, boy? | I was born without any immunities.
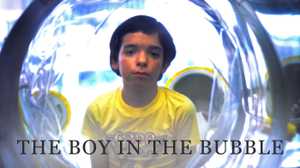
Narrator: His real name was David Phillip Vetter, but the public knew him only as "David, the boy in the bubble."
David and mother, archival: Would you clean your ears?
Narrator: Born without a working immune system, he lived his entire life isolated in a sterile plastic chamber.
News report, archival: There's a very special little boy in there -- one who's waiting to leave the hospital for good and go outside.
Narrator: To many, David's case seemed a triumph of technology over an incurable disease. To others, it was a bizarre experiment -- a symbol of medical hubris.
Bruce Jennings, Medical Ethicist: It is amazing that we can do this. But perhaps we are overstepping the bounds of our knowledge when we try to conduct experiments that are so risky, so perilous. Is it really the desire to cure and to help and to save a child? Or is it pride and egotism?
Jacqueline B. Vogel, Child Play Therapist: Incredible advances in medical technology are based on optimism. Sometimes it's warranted and sometimes it's not. But you don't always know the answer to that until way down the road.
John R. Montgomery, M.D., Pediatric Immunologist: If you take care of the patient better by doing nothing, you should do nothing. But if there is even a remote chance of success, for goodness sake, take it.
Narrator: On September 21, 1971, a suite of operating rooms in Houston's St. Luke's hospital was prepped for a delivery by caesarian section. The procedure was to take place under totally germ free conditions -- one of the first such operations ever attempted in the United States. Walls were triple scrubbed, windows sealed, and all non-essential equipment removed from the room.
The patient was Carol Ann Vetter, a 28-year-old housewife from Houston, and a carrier of a rare genetic disease that could leave her new baby without a functioning immune system.
Doctors knew that they would have to deliver the child without exposing him to a single germ.
Carol Ann Vetter Demaret, David's mother: I was wheeled into the delivery room. Everyone was standing at attention. Everything was quiet. There was no conversation; all I could see were eyes, you know, just eyes peering at me.
James H. Jones, Ph.D., Writer: Words won't be spoken. Instead a series of eye signals will trigger this well-prepared team to make the delivery. The movements, okay, will be kept to an absolute minimum to let every particle of dust settle.
Narrator: The delivering team planned to place the newborn immediately into a sterile plastic enclosure, called an "isolator."
Carol Ann Vetter Demaret: The isolator was placed to my left, right within a few inches of where I was laying. I knew it was time.
Mary Ann South, M.D., Pediatric Immunologist: Sure enough, he came out screaming. He was the healthiest kid I've ever seen born.
Raphael Wilson, Ph.D., Biological Research Scientist: He was exposed to the air in the operating room for probably no more than 20 or 30 seconds at the very most.
Narrator: Carol Ann requested that her newborn be baptized. Lead doctor Raphael Wilson, also a Catholic monk, performed the ceremony with sterile holy water.
Raphael Wilson, Ph.D.: I said, "Well, what name do you want me to give this child? And she said, "David Philip." I said, "I baptize you David Phillip in the name of the Father, and of the Son and of the Holy Spirit."
Card: A Year Earlier...
Narrator: In the autumn of 1970, immunologist Raphael Wilson arrived at Texas Children's Hospital in Houston.
Dr. Wilson had a bold new idea for how to treat one of the most baffling diseases facing pediatric immunology.
The disease -- Severe Combined Immune Deficiency, or SCID -- is a rare genetic ailment that leaves newborns defenseless against even the most common germs.
In 1970, most SCID infants did not live past their first year. By the time they were diagnosed, their bodies were so riddled with infection that nothing could be done to save them.
Mary Ann South, M.D.: There was just nothing that worked. And it was just so disheartening, one after another after another.
John R. Montgomery, M.D. : I'm an old athlete and that was an opponent who had defeated me without giving me much of a chance to fight back.
Narrator: Dr. Wilson however, believed he had discovered a way to buy time against the onset of infection in SCID infants.
His idea was to create a sterile plastic bubble, like a second womb, into which SCID babies could be placed at birth and kept germ free.
James H. Jones, Ph.D.: He was certain that if SCID children could be isolated, keeping the child physically free of germs, given time there would be a way to jumpstart their immune systems before they became damaged by infections.
Narrator: Once he had a SCID baby safely isolated, Wilson planned to repair the infant's immune system with a bone-marrow transplant, as he had already done with immune deficient mice.
A couple years before he arrived in Houston, Wilson had isolated his first human subjects -- two month-old German twins diagnosed with SCID. But before he could perform a bone marrow transplant, the twins' immune systems suddenly began working and they were released from isolation...
The experience of the German twins had been encouraging but inconclusive. What Wilson needed was a baby born into the bubble.
At the same time as Wilson arrived at Texas Children's, a young couple named Carol Ann and David Vetter were undergoing genetic counseling at the hospital.
The Vetters had a daughter, but had lost their first son to SCID when he was just seven months old. Now, they sought advice about whether to risk having another child.
In the counseling sessions, Doctors Jack Montgomery and Mary Ann South laid out the odds facing the young couple. SCID only affects male children: if the Vetters had another girl, she would be fine, but if they had a boy he would have a 50-50 chance of developing the disease.
Carol Ann Vetter Demaret: Children were very essential to our hope and to our dream of the future. We wanted to have children right away; we wanted to have as many as God would send us.
Narrator: Eager to help the Vetters, Dr. Wilson joined the counseling sessions.
Told of Wilson's research, the Vetters looked to him for reassurance.
Raphael Wilson, Ph.D.: They asked, "Well if we have another child, could you deliver this child germ free? And if the child turns out to be immune deficient could you treat the child?" "Yes," we said, "yeah, we would."
Mary Ann South, M.D.: He just swept us along with his enthusiasm. He had the confidence to say, "We can do this. We can do this."
Narrator: Wilson and his colleagues made a pledge: if the Vetters were to have a baby with SCID, the doctors would keep him free of infection long enough to perform a life-saving bone marrow transplant.
Mary Ann South, M.D.: We promised them that we would keep him "safe," in the mother's words: "Can you keep him safe? And away from the germs?" And we said, "Yes we can," and we promised that we would do that.
Within eight weeks of losing her first son, Carol Ann was pregnant again.
Mary Ada Murphy, Ph.D., Child Psychologist: It was just a couple of months and you don't get over grief of losing a child. And then somebody comes along and says you can have another boy and we can make it all right. I think almost any woman in that emotional state would have probably made the same decision.
Narrator: But the doctors' confidence had obscured another set of odds stacked even higher against the Vetters: even if their baby could be kept germ free, the chances of performing a successful transplant were small.
Bone marrow transplantation was in its infancy and required a near-perfect match between donor and recipient.
Evelyn Nelson McMillan, Writer: The doctors knew that the odds of finding a perfect sibling match were one in four. The odds of finding a match from an unrelated donor were one in hundreds of thousands. So this had always been a long shot, perhaps a longer shot than they had ever been willing to face up to.
Narrator: In the hours after his successful germ free birth, baby David was transported to the clinical research center where he was kept in protective isolation, while doctors tested him to see if he had SCID.
Elaine Potts, Nutritionist: They brought him to the unit in the little bitty bubble so that they could hook him up to get the air and everything. And he was just adorable. He was a beautiful baby. He didn't really look like a newborn. All of this black hair -- just precious.
Carol Ann Vetter Demaret: We got a call about a week after David was born and asked us to come in. We were driving in very optimistic, very hopeful. We sat down with Dr. Montgomery and Dr. South and they presented us with the news that David did, in fact, have SCID. We were devastated. We were so heartsick.
Elaine Potts, Nutritionist: Before she left the hospital, Mrs. Vetter came to see him. And she had tears in her eyes. She, of course, had just lost the other baby. And, um, she looked at me and she said, "I can't fall in love with this one and be hurt again."
Carol Ann Vetter Demaret: I felt, if I could stay distant from him, then if the worst happened I could handle it better. So I was hesitant to reach into the glove and touch him. But once I did, I was hooked for life.
Narrator: Despite his diagnosis, there was still hope for David. Unlike other SCID babies, David had remained germ free inside his bubble. The doctors now moved into the second phase of their plan: to transplant the bone marrow of David's older sister Katherine.
Evelyn Nelson McMillan: The doctors were optimistic that they could move straight forward into a successful bone marrow transplant. They had expected Katherine to be a perfect match for David. And then came the devastating news that Katherine was not a match.
Mary Ann South, M.D.: We just, we just didn't even... we didn't make plans ahead of time. If he's got this disease we'll look for a matching donor. And probably he'll match Katherine like his brother did and we'll give him the transplant and, uh, he'll be well.
John R. Montgomery, M.D.: I have to be honest that we never sat down and outlined this is what we will do "if". It was an unspoken understanding that he would match Katherine, we would transplant him, it would work, and six weeks to three months later, he would be reconstituted and come out, and we would all be joyful, and maybe famous.
Rev. Raymond Lawrence: My problem with the medical team is that they offered a bit too much hope. They offered too much and they gave too much. And they trapped themselves.
Carol Ann Vetter Demaret: I don't know if 'confused' is a good word for the doctors. We were certainly confused. There were a lot of theories. They told us that David would have to stay inside this germ free environment. Once we gathered ourselves, then we said, "Okay, now what? What happens now?"
Narrator: In what seemed like an instant, the isolator had gone from a stopgap measure to David's permanent home.
Little more than an inflated balloon, the isolator was fed with a constant flow of filtered air. Comprised of a 5-foot by 3-foot living chamber, it was connected to an even smaller supply bubble.
David had to be handled through thick black neoprene gloves, spaced at intervals throughout the isolator. Everything he ate, wore, or touched had to be sterilized with pericidic acid and placed inside steel capsules inserted through a system of air locks. Even David's doctors weren't certain it would hold up.
John R. Montgomery, M.D.: I had no idea that this situation would work for the next week, much less for the next year. I kept expecting to walk in any day and in my worst nightmare, just see him falling apart.
Narrator: The medical team now faced a choice: they could leave David in the bubble hoping that his immune system might kick in or a new treatment be found -- or they could take him out and let his disease run its natural course.
In June 1973 when David was 18 months old the chairman of the pediatrics department decided it was time to remove him from the bubble.
Raphael Wilson, Ph.D.: He essentially said, "Get this over with." His point was that you have a case to treat. You use the best tools you have at the present time, and if it doesn't work it doesn't work. My point was that this would be the approach with a child who was sick. David was not sick. So I said to him, "If you think it should be terminated, you terminate this case. You're chairman of the department, but I'm not going to do it." And that was -- that was the end of that.
Narrator: The faith David's doctors placed in technology reflected the times. By the early 1970s, American medicine itself had undergone a significant cultural shift.
Following World War II, important advances in medical technology -- from the iron lung to the artificial heart -- had emboldened doctors.
Bruce Jennings: By 1971 we in the United States were well along in a remarkable period of medical progress. Medicine was on a roll. And in that climate it was natural for physicians and researchers to want to take up any condition which was incurable and treat it as a challenge -- treat it as an enemy to be defeated.
Narrator: David's doctors were especially prone to the lure of technology. Texas Medical Center, home to Texas Children's, was the epicenter of medical innovation in the United States, from the separation of conjoined twins to major advances in heart transplant surgery.
Walter Cronkite, Archival: Below me, a delicate operation is taking place: an operation on the human heart. The surgeon is Dr. Michael Ellis Debacle, the world-renowned Houston specialist.
Jacqueline B. Vogel: Lots of wonderful things happened at the Texas Medical Center. It's an amazing institution with a history of many amazing breakthroughs. Lots of us that were involved with David's care really assumed that big breakthroughs were possible in terms of immune deficiency.
Raphael Wilson, Ph.D.: So, there was an element of hope, expectation, of optimism -- that we're working on this but we're not there yet.
Narrator: Now banking on a future medical breakthrough, David's doctors threw themselves into a vigorous research effort into SCID. They scoured the world for leads on how to perform a transplant without matching bone marrow -- and meticulously studied David himself to better understand the human immune system.
Mary Ann South, M.D.: Finally, finally here was something that we had to work with. We were able to watch the progression of this disease uninfected for the first time in history.
Nurses' chart notes: The immunization experiment will include the following: bacteriophage will be given intravenously. Small blood samples will be taken at three days, five days, seven days, 14 days, 21 days ...
James H. Jones: David was a research subject as well as a patient. And those two roles became blurred. Here is a child who, over time, has so many punctures that his feet started to look like pincushions.
Rev. Raymond Lawrence: When I first saw David I was very disturbed -- I think deeply disturbed -- by the fact that he was in this laboratory tube. I was not comfortable. I mean, I felt like I was visiting a rat in a cage.
Raphael Wilson, Ph.D.: He was not a guinea pig in the sense that we delivered him with the intent of having an experimental subject. But we had to continue our research because we were working in an area where there was no previous experience.
Narrator: While research went forward on David, Wilson and his colleagues spoke at conferences, wrote articles, and appeared in the media, painting a cheerful picture of David's life in the bubble.
Archival, press conference: Dr. Wilson, how do you assess his development?
Raphael Wilson, archival: Physically, he is well developed. He is strong. His muscular development is normal. His psychological development, if anything, is ahead.
Narrator: Primed by David's doctors and the hospital's public relations department, the media eagerly reported what one newspaper called "the miracle in Houston".
Archival, news: There's a very special little boy here: one who is waiting to leave the hospital for good and go outside.
James H. Jones, Ph.D.: The interest in David from his germ free birth forward built over time, and he became a celebrity in his own right.
Archival: News stories don't mention his last name in order to give some privacy to a little boy and his family, but the story of David, the boy who lives in a bubble, has been told around the world.
Evelyn Nelson McMillan: The story told over and over again to the American public in David's early years was that this was very successful, that this was a very happy, intelligent, active, thriving child, and that the cure was just coming right around the corner.
Archival: He seems very happy and active with an abundance of toys and love here which makes the waiting easier.
Narrator: The upbeat news was not entirely unfounded. While just a few months old, David had been allowed to leave the hospital for his parents' home an hour away.
Carol Ann Vetter Demaret: David never questioned in the early years, why he was in a bubble. It was routine for him to have his mother hold him with black gloves on. In the beginning, you know, children -- their needs are very simple, so David's needs were very simple.
Narrator: But as months turned into years, there was little real progress in the search for a cure. Bone marrow registries in Europe had not come up with a matching donor for David, and there were no breakthroughs on a non-matching transplant.
John R. Montgomery, M.D.: Nothing seemed to offer real hope and most of the procedures offered real danger, and as long as the isolator was working we didn't have to do anything.
Narrator: By David's third birthday in September 1974, there had been a significant shift in how his doctors saw his case. The original promise to quickly cure David had been replaced by what Dr. Wilson himself called "a holding pattern".
Evelyn Nelson McMillan: The bubble was successful for David. It did protect him. He was a living, breathing, laughing, talking child. And now they had no way out. There was no way to conscientiously, in their thinking, remove this happy child from this protective environment and expose him to the dangers of the world. How do you kill a child?
University of Virginia conference, archival: Our case today has to do with a little boy who has spent a number of years now in an isolator.
Narrator: In the winter of 1975, doctors held a conference at the University of Virginia on the now-famous case of the Boy in the Bubble.
Raphael Wilson, University of Virginia conference, archival: Can you hear me? Am I coming through all right?
The featured speaker was Raphael Wilson, himself.
Raphael Wilson, University of Virginia conference, archival: May I have the first slide?
Narrator: Wilson began with a detailed lecture on the mechanics of the isolator.
Raphael Wilson, University of Virginia conference, archival: When he was two years old, we built him this playroom, which has solid plexiglass walls.
James H. Jones: What happens very quickly, questions are raised spontaneously from the audience, questions that had never been asked before.
University of Virginia conference, archival: Well, I share, I'm sure, with a lot of people here extreme admiration for the technological sophistication of what's been done for David, but I'm very deeply troubled as I think many of us are, about when he begins to ask, "What have you done to me?"
What is our ethical position if and when David says, as he may well do somewhere down the line, "I've had enough. I'm coming out of here; just stand aside."
Raphael Wilson, Ph.D.: I really felt that sometimes their questions were very inappropriate in the sense that they were based on, on uh, situations that simply did not exist.
Raphael Wilson, Ph.D., archival Having been raised in this from the outset, he can no more think of removing himself from the bubble than shedding his skin.
John R. Montgomery, M.D.: We were doing all right. Why do we have to worry about something that maybe years down the road, that may never occur, and that probably, if you look at what we have done over the past two or three years of taking care of David, when the problem comes up, we'll solve it?
Evelyn Nelson McMillan: They were totally unwilling to look ahead. They were happy with the present, with how well things were going. And they were unwilling to face the fact that this very intelligent child is going to grow into an awareness of his situation and is going to question it.
David Vetter, archival: A, B, C, D, E, F, G ... [inaudible]
Carol Ann Vetter Demaret, archival: That's very good, sweetheart!
Narrator: In his first few years of life, David had thrived in isolation.
Patricia M. Bealmear, Ph.D., Researcher: It was amazing to see him develop. When he was about 21 months old, he was playing with this little red wagon and he was turning the wheels and he says, "What is that in there?" ... his first real sentence. See, he was just amazing how much he could learn -- how quickly.
Narrator: By the time he was four, however, David was presenting a whole new set of challenges.
It was one thing to keep a toddler in the bubble, another to contain an energetic boy.
Patricia M. Bealmear, Ph.D.: The older he got, the more active he was you know, you had to be super, super careful.
Carol Ann Vetter Demaret, archival: What's wrong with the edges on this lid?
David Vetter, archival: They're sharp.
Carol Ann Vetter Demaret, archival: They're very sharp. And what can they do to you?
David Vetter, archival: Cut.
Carol Ann Vetter Demaret, archival: Cut.
Patricia M. Bealmear, Ph.D.: One time after they had taken his blood sample, he had kept one of the little butterflies that they used to insert into the vein, and they didn't ... nobody noticed it. And that evening, all of a sudden he dashed up the stairs into the bubble and he was going all over the place.
And I thought what are you doing? And, like here was this little butterfly and he was poking holes in the isolator. This was the only time he had any control. He could do something, you know, to the isolator that would get everybody going.
Narrator: Dr. Wilson decided that the only way to control David was to make him more aware of the dangers posed by the outside world.
Raphael Wilson, Ph.D.: I said, what happened to your isolator today? He said, "Somebody made a hole in it." I said, "Yeah, I know somebody made a hole. Who made the hole?" And he thought for a moment and said, "I made the hole." I said, "Okay David, I want to tell you why making a hole in the isolator is very bad." I said, "Do you know what will happen if you make a hole in the isolator?" And he said no. "Little bugs will get in ... little tiny, tiny bugs that you can't even see. But they're bad; they'll make you sick. If they get in, they'll make you hurt all over." So I said, "They'll hurt your eyes, they'll hurt your ears..." and I went down his whole anatomy.
And I said, "Now do you understand why it's important that you don't make any holes in the isolator?" Yeah, he understood. This was the first time that we had any conversation with him about the reasons for his isolation.
Nurses chart notes: I transferred linen and took trash out. While I was cleaning up, a patient walked up to door and stated: "Will he have to live in that thing for the rest of his life?" The speaker system was on at that time; I am positive David heard the statement clearly. He reacted with silence and sucked his thumb.
Narrator: With greater awareness, David began to comprehend how different his life was from others.
Jacqueline B. Vogel: I think he became more introspective, quieter. When I would come to visit and he would really have very little to say at all. He would sit on his knees and rock back and forth.
Narrator: Child psychologist Mary Murphy began to work intensively with David when he was five.
Mary Ada Murphy: I really liked him. I really thought he was delightful, yet at the same time, I felt so sad. I thought, "Oh my god, how can this bright, bright child survive in this little space?"
Narrator: As Murphy spent more time with David, she began to discover new ways in which his confinement was affecting him.
Mary Ada Murphy, Ph.D.: There were so many things he couldn't understand -- like wind -- he absolutely could not understand it. I made the pinwheel and put it on his blower. But still he did not understand the wind outside. He saw the world as flat. There was nothing behind anything. I said something about leaves and he said, "Well trees didn't have leaves; they were a brown rectangle and a green oval." And so it was pouring down rain and so I went out and tore a branch off the tree to show him and he just go so excited about that. And he just couldn't believe it.
Narrator: To relieve his sense of isolation, Murphy encouraged David to escape his bubble using his imagination.
James H. Jones, Ph.D.: They pretended that they were on space odysseys, -- places that transcended his isolator. And they had made great adventures where they explored other planets, in which he got to be a swashbuckling space captain.
Mary Ada Murphy, Ph.D.: Night after night we would make all these trips all through the universe. He was the pilot and I was his copilot. And he would always protect me and bring me back safe.
News, archival: What're your hopes for him? Well we're very optimistic about David's problem, with all his genius doctors working on his case all over the world, we truly believe that one day, soon, David will be able to come out.
Narrator: As the Vetters waited for a cure, research on David began to produce results. Immunologists had learned how SCID suppressed the immune system. Hematologists learned about the properties of germ free blood, and psychologists learned about the human response to physical isolation. While the scientific harvest had been rich, it had done little to help David. The barrier to a bone marrow transplant, or any other possible cure, remained as insurmountable as ever. Then, in 1975, Dr. Wilson had a brainstorm: he would get NASA to design and build a miniature space suit for David.
News, archival: Right now, he's been restrained to his little bubble world and he's never really been able to get out and walk and play and maybe go to the zoo. But this would give him a much more intimate touch with the real world.
After more than two years of development, David prepared to enter the space suit for the first time.
Dorothy M. Johnson, R.N.: His mother was at one end of the tunnel which he would come out of, and she kept encouraging him to come on, come on... At the very last minute, he decided, "Well maybe this wasn't such a good idea. Maybe I'll just stay in my little bubble."
Narrator: Finally coaxed down a 10-foot long tunnel into the suit, David took his first tentative steps outside the bubble.
Carol Ann Vetter Demaret: David was in awe of everything around him, he was looking right and left all the time. He was fascinated by the simple things like the faucet in the lavatory.
After a few walks in the hospital David was allowed to explore the outdoors for the first time in his life.
News, archival: A specially designed suit allows him to experience the world. ... The mobile unit has given David a chance to explore the outside world. And in a recent outing, he playfully sprayed his mother with a garden hose. ... The ever-smiling effervescent youngster took his first walk in the outside world as he watered the yard and played with the family dog.
James H. Jones, Ph.D.: This is a PR dream. But David behind the cameras, where no one can see, is very afraid of getting in that spacesuit.
Dorothy M. Johnson: He was very, very frightened. He would complain that it was hot or that it was too small, or something.
Mary Ada Murphy, Ph.D.: You know, he wanted out, but he was scared to death that the germs would come in. I mean the world is full of germs. The fear he had -- I mean that fear was instilled in him from day one.
Narrator: After only six walks, David refused to get back in the space suit and it was permanently retired.
Jacqueline B. Vogel: It was disappointing; it was very disappointing. I'm not sure what I imagined; I just didn't imagine it would be that difficult. It made it very clear that trying to help him experience the wider world was going to be ever so much more difficult than anybody expected.
Mary Ann South, M.D., archival: Everyone involved in David's care has felt trapped by the situation at one time or another. Because we do feel that it's a problem we can't turn off and walk away from.
Narrator: David's doctors had always promised to keep him safe until they could find a cure. But after years of frustration, they each left to pursue their careers elsewhere. Dr. South was the first to go.
Mary Ann South, M.D.: My reasoning was: I would not leave in spirit. The work is going to go on. I've done what I can do for David.
Narrator: Jack Montgomery left a few years later.
John R. Montgomery, M.D.: I was not contributing in any way to a solution to David's problem. I was just keeping things going.
In the spring of 1976, shortly before David turned five, Raphael Wilson suffered a major heart attack. David was taken down the hall to visit him.
Raphael Wilson, Ph.D.: They nurses wheeled his isolator into my room. David took one look at me and started to scream. His worst fears were coming to light. Something could happen to me so that I wouldn't be able to take care of him.
Narrator: After his recovery, Wilson informed David that he too would be leaving Houston.
James H. Jones, Ph.D.: The three people who are to keep him alive are no longer on his case. David understood that his life depended on those individuals finding him a cure. And when each of those individuals, from his perspective, abandons him, he must have understood that his future took a turn for the worst.
Nurses' chart notes:
- David was very quiet today. Sucking his thumb constantly and rocking back and forth...
- He can't say why he is unhappy but that he definitely is.
- David seemed upset when I arrived -- he was repeating out loud, "One, two, three, four, I can't take this anymore."
- David did not talk openly about being unhappy but did want me to sit and hold his hand most of the session...
- In books and stories, David keeps coming back to themes of death. This is increasingly prevalent in how David responds to stories he sees on television.
- The entire group felt sadly that David's anxieties are intensifying rapidly and that his anxieties are getting beyond his control.
Dorothy M. Johnson, R.N.: You would go in the room and he would be just sitting there, staring into space. You would say something to him and he would respond: "I don't want to talk; leave, you know, get out." There were times when I really wondered, "Why are we doing this? Why are we putting this child through all of this?"
Mary Ada Murphy, Ph.D.: It was the mental anguish of knowing that tomorrow is just going to be like today, only worse. He had no choices, and his hormones were kicking in and he felt that everybody was deserting him, which in reality, they pretty much were.
Well, he always had nightmares. He would tell me what his nightmares were. We would reenact them and I'd say now what we're going to do, we're going to change the end. The "King of Germs" -- that was a recurring one. The King of Germs was going to get him, and the King of Germs had all these wives and we could slay the wives and we would kill the people working for the king, but we never could get to the king. We just couldn't get the king. And if you didn't get the King of the Germs, the dream goes on.
William T. Shearer, M.D.: Here he was, inside of this system. Something obviously had to be done. It just seemed to be going on and on and on. And one had to say, "When is this going to stop?"
In the fall of 1978, immunologist William Shearer was put in charge of David's case.
James H. Jones, Ph.D.: Dr. Shearer saw David with a fresh vision. He was in no sense hostage to the original set of attitudes and hopes you know that put David in that isolator. What he saw quite simply was a failed experiment.
William T. Shearer, M.D.: My feelings were to advise the parents of the options and to really draw a focus to a decision.
Narrator: Shearer had David examined by a team of psychiatrists. Their report was unequivocal: David would continue to deteriorate as long as he remained in the bubble.
Dr. Shearer's Case Notes: I have shared the preliminary findings with the Vetters -- that David has extraordinary fears and anxieties. My recommendation to Mr. and Mrs. Vetter was that David be removed from the isolator system. The Vetters appeared to be shaken by this discussion.
Carol Ann Vetter Demaret: I remember the conversation. And he was -- he was very blunt. It was suggested that David be removed from the bubble and then just be treated accordingly. Well I knew that that was, um, certain death.
Narrator: Panicked by Dr. Shearer's recommendation, the Vetters turned to David's original doctors for advice. All three were outraged.
John R. Montgomery, M.D.: For these many years we had had a success story, and should this happen, this would be the ultimate declaration that it was a failure that the whole thing was a failure.
Mary Ann South, M.D.: None of the three of us were going to just sit by and let this happen. And we assured them that nobody could take David out of the isolator until they consented.
Narrator: Steeled by the doctors' resolve, the Vetters demanded that Dr. Shearer maintain David in the bubble until a cure could be found.
Bruce Jennings: To continue to say, "This is a bridge, we just have to wait longer; this is a bridge, we just have to wait longer; be patient..." is wrong. It's depriving the parents of the choice that they have to make: to confront the options that have to be confronted. If you continue to pretend that this treatment or this environment, this plastic bubble has not turned into a prison.
In the spring of 1981, when David was nine, Shearer decided to discharge him to his parents' full-time care. Surrounded by his family at home, David's mood lightened for a time. But soon, even his parents began to be concerned.
Carol Ann Vetter Demaret: I think, for us, the summers were especially hard. I would notice that David would spend a lot of time gazing outside. And he would see young boys on bicycles or he would see kids tumbling in the grass. I sensed a sadness to him. The time was coming soon where, you know, something would have to be done.
Narrator: Then, just as the situation reached bottom, came hints of the long sought after breakthrough. A team of researchers in Boston announced that they had developed a way to safely transplant incompatible bone marrow. The Boston procedure offered hope that Katherine's bone marrow could finally be used to kick-start David's immune system.
James H. Jones, Ph.D.: The procedure is experimental; it has not been proven to be efficacious, but after nothing on the radar screen, this is the first bleep of hope.
Carol Ann Vetter Demaret: It was a chance; if it didn't work, he would still be okay. David knew that; that's how we explained it to him. That's how science explained it to us.
Narrator: In the early morning hours of October 21, 1983, Dr. Shearer transfused two ounces of Katherine's bone marrow into David's body.
Carol Ann Vetter Demaret: We did fantasize. We did think about how all of that was behind us, and how exuberant we were going to be when we could touch David for the very first time.
News, archival: Hello, everybody. For 12 years we've known the youngster simply as "David the bubble boy." But early this morning, doctors operated on David. And our medical reporter Christie Meyers is with us now with the good news that this operation may mean that David someday can leave that bubble.
John R. Montgomery, M.D.: The tone was very optimistic, everything seems to be going well. You know, you sort of went around with your fingers crossed saying, "No news is good news." And then came the bad news.
Carol Ann Vetter Demaret: It was New Year's Eve when I took his temperature and it seemed elevated. I called the hospital and I said, "You know -- something strange -- David has a little temperature."
Narrator: In the days that followed, David's temperature spiked as high as 105 degrees. He began hemorrhaging from his intestines and vomiting blood. Dr. Shearer struggled to treat him inside the bubble.
William T. Shearer, M.D.: He was to the point where his fever could not be controlled. His intestinal bleeding could not be controlled. It was just impossible. This contraption that protected him was now his greatest threat. It had to go; it had to go.
Narrator: Shearer told David that it was time to leave his bubble. On February 7, 1984, David began to make his way out.
Mary Ada Murphy, Ph.D.: He crawled into the supply bubble and it took all his effort. And Shearer put his hands under David's arms and pulled him out and laid him on the gurney.
Narrator: David was wheeled to a sterile room. Freed from isolation for the first time in his life, even the smallest things seemed wondrous.
Mary Ada Murphy, Ph.D.: The sun was coming through in little streams through the Venetian blind and he saw what he called -- he said there were minute snowflakes -- and it was actually the dust from the linen. And he was there, and he was feeling comfortable and he was playing with the snowflakes.
Narrator: But David's fever and bleeding persisted and his condition gradually deteriorated. Finally, he lapsed into a coma. On February 22nd, 1984, David's parents were brought in to see him.
Carol Ann Vetter Demaret: I looked over to the side of David's room, and there was a physician standing. And I asked him if I could remove my glove and touch David, and he nodded yes. So I walked over to David, and I took my glove off of my hand, and I stroked the back of his hand, for the first and last time.
At 8pm that night, David was pronounced dead. He was twelve years old.
William T. Shearer, M.D.: It came, and it happened, and there was no emergency, there was no crew brought in to resuscitate. Uh, there were no tubes inserted. We had decided that it was not going to happen. This was going to be a dignified death. And it was.
Narrator: It wasn't until David's autopsy that the cause of his death became known. Katherine's bone marrow had contained traces of a dormant virus. Once inside David's defenseless body, the virus had spread rapidly, producing hundreds of cancerous tumors.
Proof that a virus can cause cancer was probably the most important of the many medical insights that emerged from David's case.
If these discoveries had done little to help David, they would help to treat thousands of immune compromised children in the future.
Yet some continued to question whether David himself had borne too high a price for the advancement of medicine.
Rev. Raymond Lawrence: David was almost certainly the first human guinea pig in history. The first human being to live their entire lives in a laboratory capsule. And I don't think we ought to do that again.
John R. Montgomery, M.D.: A team of dedicated and courageous people, including David and his family, set out to treat an incurable disease. And in the process, they gave him twelve years of good life that he would not have had otherwise.
Carol Ann Vetter Demaret: I don't have regret and I don't have blame. Any parent who has lost a child wonders if their brief life has meant something to the world, and science has said to me: yes.
Evelyn Nelson McMillan: As a society we have yet to confront these issues. We're still amazed and baffled by our technology. We still chase after things; we still deploy the technology entirely too frequently without having an exit strategy.
James H. Jones, Ph.D.: Scientific curiosity, the desire to test technology, to see what is possible, has to be tempered with a very deep respect for our need to be human.
Card: More than 90 percent of infants diagnosed with SCID are now successfully treated with bone marrow transplants. Long-term isolation is no longer offered as a treatment option.