
The common wood frog has taught bioengineers like Boris Rubinsky much about biological tolerances to freezing. 
This may look like a set of steak knives, but it's actually ice crystals that form in a physiological saline solution. 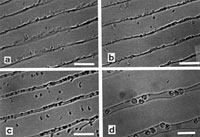
These images show red blood cells between ice crystals, at different temperatures below freezing. (A) is the lowest subfreezing temperature, (D) the highest. Note how the cells shrink as they become exposed to lower temperatures. 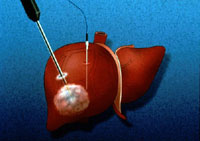
In this animation still, freezing propagates out from the tip of a cryosurgical probe inserted into a liver. Next to the probe is a thermocouple needle to measure temperature. 
This is the first-ever ultrasound image of a frozen lesion in a liver. The arrows point to the margin of the frozen lesion, which appears dark because it reflects the ultrasound pressure waves. |
Frogs that survive freezing excite our imagination with visions of immortality. Underlining this excitement is the unexpected: our experience tells us that freezing kills. We've all read news stories of people who have lost fingers or toes to extreme cold, or even their lives. Thus, a whole animal that can survive freezing comes as a shock. Yet during the past two decades we have also read or even experienced the successes of in vitro fertilization, which involves the routine storage of sperm and embryos in a frozen state at cryogenic temperatures (-40°F or lower). So why is the survival of a frozen frog at 26°F surprising? Thoroughly confused? You should be. Freezing has a yin-yang effect on biological materials—it can both preserve and destroy tissue. This paradoxical nature has led to two different fields of science and medicine built around freezing: cryopreservation and cryosurgery. Surviving the deep freezeLife is a complex set of electrochemical reactions. The rate at which chemical reactions take place depends on temperature, and usually the lower the temperature the lower the rate. At absolute zero Kelvin (-460°F), the rate is zero. Therefore, lowering the temperature of biological materials such as cells, organs, or entire organisms to absolute zero causes life to stop indefinitely. If a person or his or her body parts could survive the excursion to absolute zero and back, scientists and physicians could theoretically use such freezing as a vehicle to transport that person or parts to any point in the future. Because we humans are mostly water, however, any journey into the supercool is physically traumatic. At about 31°F, the water in our bodies begins to freeze. It starts at this temperature (rather than 32°F) because biological water is in the form of a solution, mainly of ions or charged atoms. The survival of any cells during freezing depends at minimum on the rate the temperature changes. For most organisms, even the slowest cooling results in an assault on their cells that is just too great. Resulting cell damage is related to the dissolved substances or solutes in biological water, to the cell membrane properties, and to the fact that ice has a very tight crystallographic structure and cannot contain solutes. When biological materials freeze, the solution between cells usually freezes first. Solutes found in the original solution are ejected and concentrated in the unfrozen space between the ice crystals. Cells usually remain unfrozen though supercooled. In order to balance out the resulting difference in potential energy between the inside and outside of the cell, water leaves the cell through the cell membrane. Inside the cell, this loss of water causes an increase in the ionic concentration and leads to chemical damage. Interestingly, ions, not ice crystals, trigger cell injury during freezing. Theoretically, an infinitely fast rate to absolute zero would eliminate this harm. This is not possible, of course, and at higher cooling rates the supercooling of water in cells causes ice to form within those cells, which also brings about damage. Natural antifreezesCells in freeze-tolerant wood frogs experience the same mechanism of freezing injury as any other creatures' cells. The frogs freeze very slowly to a temperature often several degrees below freezing. This should destroy the frog's cells, yet those cells and the frog as a whole survive. How? A primary mechanism is through the production of glucose and its incorporation in the frog's cell. By lowering the amount of water that leaves the cell during freezing, the glucose offers protection against the rise in ionic concentration and excessive cell shrinkage, thereby reducing chemical harm. While the wood frog spent millions of years perfecting the use of such chemicals, scientists in the field of cryobiology discovered the mechanism over just a few years. Today, every known cryopreservation protocol of sperm, embryos, red blood cells—literally every cell that survives freezing—employs a similar mechanism. The chemical substances that experts introduce into the cell are known as "cryoprotectants." These include glycerol, ethylene glycol, and dimethyl sulfoxide, among others. But if cells can be preserved at cryogenic temperatures, why not whole organs or whole frogs? The reason is that in organs and tissues the cells are in a precise matrix, which the cell shrinkage caused by freezing usually disrupts. This is why we can preserve cells but not organs. The frogs have evolved to produce just the right composition of cryoprotectants and gross tissue properties that allow them to survive freezing at the temperatures they experience in nature. They cannot survive freezing at lower temperatures. This is the key attribute of evolution: it solves only the challenge an organism encounters and nothing else. Inspired by the way wood frogs survive freezing, my research team developed a cryopreservation protocol for mammalian liver. We successfully preserved a liver in a frozen state and then transplanted it into an animal that survived. This was the first time this had been done with any organ, and we're now successfully cryopreserving organs for hours to days. So far we have achieved only what the frogs can achieve, however: cryopreservation at high subzero temperatures. At temperatures lower than a few degrees Fahrenheit below freezing, neither the organs nor the frogs survive. If we could follow such a protocol at cryogenic temperatures and thereby slow chemical reactions to negligible levels, we could conceivably preserve organs for months or even years. That is our goal. Attack of the frozen probesWithout cryoprotectants, cells in tissue usually do not survive freezing. This gives rise, however, to the other application of freezing, cryosurgery, a surgical technique in which doctors use freezing to destroy undesirable tissues. The history of cryosurgery is closely intertwined with developments in low-temperature physics, engineering, and instrumentation made in the 19th century. Around 1845, following earlier successes by others in achieving very low temperatures, the chemist and physicist Michael Faraday reached a temperature of -166°F by mixing solid carbon dioxide and alcohol in a vacuum. During the same period, James Arnott of Brighton, England, who is recognized as the first physician to make use of freezing for cancer treatment, began applying such low temperatures in medicine. In several reports published between 1845 and 1851, he describes the use of a solution of crushed ice and sodium chloride to freeze advanced cancers in the breast and uterine cavity. Modern cryosurgery began in the 1960s through the work of the neurosurgeon Irving Cooper. Together with engineer Arnold Lee, he built a cryosurgical probe capable of freezing brain tissue. Cooper's cryosurgery was the first minimally invasive surgical technique of modern medicine, and his probe is essentially the prototype from which every subsequent device of this nature has been built. The probe is a needle-like instrument cooled with a cryogen that flows through the probe to its tip and back. Doctors insert the tip into the undesirable tissue, which is then frozen in the hope that freezing will destroy it. By 1970, physicians were using the technique to destroy virtually every unwanted tissue throughout the body. Despite the procedure's success, it proved difficult to control the extent of freezing. Because freezing propagates from the probe outward, the surgeon could not visually determine the extent of the tissue affected, unlike in more conventional surgical resection techniques. Therefore, while surgeons could apply cryosurgical probes at precise locations, the probes' effect on tissues was not precise. Physicians soon began bemoaning this lack of precision, and the method declined in use. By the early 1980s, laser techniques began to replace cryosurgery, which reverted to its original applications, dermatology and gynecology. Seeing the extent of the damageCryosurgery experienced a revival in the early 1980s after Dr. Gary Onik, medical director of clinical imaging at Florida Hospital, and I recognized that specialists could use medical imaging to detect the extent of freezing inside the body. This led us to develop the field of imaging-monitored cryosurgery (IMC). As with other advances in cryosurgery, IMC's emergence grew out of preceding technological innovations. Foremost among these was the ability to image the whole human body, certainly one of the most important developments in 20th-century medicine. Specifically, experts in the 1970s began coupling advances in computers and microprocessors with other technologies to develop X-ray computed tomography, magnetic resonance imaging, and ultrasound. The ability to view freezing inside the body and thereby sculpt the frozen lesion to the shape of a tumor led in turn to the need for several cryosurgical probes that surgeons could use simultaneously to achieve a desired ice shape. Together with our colleagues, Dr. Onik and I developed single-unit, multiple-probe cryosurgical systems, which along with imaging became the basis for the practice of IMC from the 1990s to the present. Currently, IMC is a clinically accepted technique for the treatment of every type of solid tumor, including liver, prostate, kidney, lung, and breast cancer, with hundreds of sites and tens of thousands patients treated with this technique in the United States alone.
Thus, while excessive freezing kills the wood frog, when used in IMC it is
saving lives. And I'm happy to report that the work has come full circle:
inspired by IMC, my research team has used magnetic resonance imaging to
noninvasively study the process of freezing in the wood frog, leading to an
understanding of the fundamentals underlying this animal's extraordinary
survival strategy.
|
||||||||||
|
|
|||||||||||
|
© | Created April 2005 |
|||||||||||
