|
|
| ||||||||||||
|
|
 |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
At medical meetings I often lecture on altitude illness, and a small group of people is always waiting for me before my lecture with single-minded questions. "I am going to climb Kilimanjaro (or Denali or Everest, etc.)," they state, then ask, "How can I improve the probability that I will make it to the top? What can I do to get ready for the altitude?" I have always chosen to steal a line from my mentor and colleague Dr. Peter Hackett, who answers such questions with a smug but honest "Choose your parents well." Genes do indeed play an enormous role in determining who will do well at high altitude and who will not. Performance depends on many physiological factors, some of which probably remain unknown. For years, scientists and physiologists have toyed with measuring specific parameters to predetermine whether someone is likely to summit the world's highest peaks. Unfortunately, no laboratory test to date has proved a reliable predictor, but these studies do point to several physiological factors that may play a role. Test casesIn the 1980s, high-altitude physiologists began focusing on a factor called HVR, High-altitude Ventilatory Response. If I suddenly sucked most of the air out of the room you're in, you might reflexively breathe more rapidly than others would in response to the decreased oxygen reaching your body's tissues (a condition technically known as hypoxia). People who breathe more rapidly are said to have a brisk response, while those who don't are said to have a blunted response. It's well known that acclimatization to altitude strongly depends on an increase in ventilation. So researchers thought that people who respond briskly to hypoxia might be better suited to high-altitude climbing. The studies do show that people with brisk responses may have an easier time acclimatizing, but they don't hold the key to predicting if climbers will make it up mountains. Some people who exhibited blunted responses still summited great mountains without difficulty. Acute Mountain Sickness, a debilitating mix of headaches, nausea, and breathlessness, is triggered by low blood oxygen levels. Even at sea level, people naturally have different levels of oxygen in their arterial blood; the higher the oxygen saturation, the redder your blood. Researchers suspected that people with relatively low blood oxygen levels would have a tougher time climbing high. The advent of small pulse oximeters, which clip onto a finger and noninvasively measure the color and corresponding oxygen saturation of blood, meant that virtually anyone could monitor his or her own arterial oxygen saturation. Could this simple test, conducted before climbers left for a mountain, predict if they would do well? Again, as with HVR, while there was some correlation, many climbers with low readings still managed to get to the top of the world's highest mountains. Climbers of the future may have their cells tested for genetic evidence of “the right stuff.”
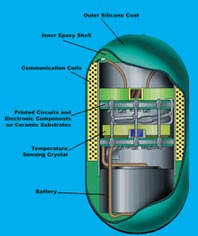
Another simple test that may have some predictive value measures the volume of a climber's lungs. Called Forced Vital Capacity (FVC), this test measures lung capacity as subjects exhale as rapidly as possible. Climbers with large FVC, who can move a lot of air quickly in and out of their lungs, seem to perform better at altitude. Yet there are so many variables affecting performance while climbing that this test alone may not be predictive for an individual. Looking to the future, it's possible that we will one day use genetic markers to determine who is likely to do well at high altitudes. There already have been a few papers published on the genetic components of high-altitude pulmonary edema (HAPE), a life-threatening condition in which the air sacs, or alveoli, of the lungs burst and the lungs fill with fluid. These studies have looked at certain genes involved in nitric oxide production, which is associated with HAPE. Climbers of the future may have their mouths swabbed and their cells tested for genetic evidence of "the right stuff" before going to big mountains. Taking the pillIs a climber's ability to maintain a relatively stable core body temperature important to his or her success in summiting a mountain like Denali, where windchill temperature can drop to -148°F? Surprisingly few studies have been done that look at core body temperatures in exercising climbers at high altitude and in extreme cold. To conduct such a study, our team would need some special technology. Contrary to popular belief, a standard fever thermometer doesn't measure true core temperature. A thermometer placed in the mouth is measuring just that, the temperature of the mouth. Breathing can affect oral temperatures, especially in the frigid air of a mountain like Denali. A more reliable means for obtaining something close to core temperature is the use of rectal thermometers or rectal temperature probes. Understandably, few climbers will permit this form of monitoring for the sake of science! So we set out on the expedition with extraordinary little pills that would, for the first time, measure core temperature in exercising climbers. The thermal radio pill was developed in the 1980s under a grant from NASA, which was interested in using the pills to monitor astronauts, particularly during EVA (Extra Vehicular Activity, or space walking). The pill contains a temperature-sensitive quartz crystal oscillator and a miniature silver oxide battery, all encased in epoxy and covered with silicon. The pill transmits a continuous radio signal to a small handheld device that records continuous temperature measurements. The pill will transmit as long as it remains in the intestinal tract, typically one to two days. A surprise on DenaliThe radio pill gave us insight into the tremendous core temperature swings climbers can experience. Contrary to the image of a high-altitude climber always being cold, it is more accurate to say that climbers are usually either freezing or frying. The ambient temperature may be -30°F, or far colder, but climbers produce massive amounts of metabolic heat during strenuous ascents. What's more, they are dressed for the cold. It's difficult to thermoregulate—maintain a stable core temperature—by shedding clothing when you are encumbered with a heavy load of climbing equipment, including climbing harness, rescue gear, backpack, and sled. Often the work required to reduce clothing is simply too great, and climbers will opt to continue onward even if they feel uncomfortably hot. The most important adaptation we human beings have to cold is behavioral.
We knew that climbers' core temperatures were likely to vary, but the large variations in John Grunsfeld's core temperature surprised all of us. During periods of heavy exertion, his core temperature rose as high as 103°F. And when he stopped to rest in the bone-chilling winds, his core temperature plummeted as low as 95.5°F—just a fraction of a degree away from hypothermia, the state in which the body's vital organs begin to shut down. We were originally suspicious of a recording artifact or error, but later discussions with cold physiologists confirmed that the fluctuations we witnessed were certainly possible. What could explain John's plunging core temperature? When he was exercising strenuously, the blood vessels in his skin and muscles were dilated. (Both exercise and heat cause vaso-dilation.) When he stopped for a break, his skin was wet with sweat, particularly on his back, where his pack precluded much evaporation. Upon resting and removing his pack, his body lost a tremendous amount of heat through convection—both windchill and blood flow through dilated vessels. Wind hitting his wet fleece would produce a profound evaporative cooling effect. If John chose to sit on a rock, there would also be conductive heat loss into the rock. Although his insulation protected him somewhat, the insulation would get compressed when he sat on it, and heat loss would be inevitable. And, of course, an immediate and substantial drop in metabolic heat output occurred when he stopped climbing. A complicated pictureIt's hard to say exactly why John Grunsfeld's core temperature fluctuated wildly while Caitlin Palmer's did not. It is known that the most important adaptation we human beings have to cold is behavioral: our ability to use our brains and put on protective clothing, seek shelter from the elements, and eat and drink to keep our bodies warm. While John is an experienced climber, Caitlin is a professional guide with vastly more experience dealing with the rigors of Denali. She has probably learned over the years how to fine-tune her thermal microclimate. She likely makes very subtle changes in her exercise rate to keep herself from overheating and better regulates her protective clothing layers. She interacts optimally with her gear, minimizing effort and maximizing ventilation and cooling when necessary. Her high level of fitness also allows her to climb with relatively little effort and better control of her metabolic heat output and sweating.
Were the fluctuations in John's core temperature the decisive factor in his not making it to the top of Denali?* Many signs showed that it wouldn't be prudent for John to attempt to summit. These included his headache and low blood oxygen levels, a cough that might have been an early indication of HAPE, his fatigue, and his dangerous swings toward hyper- and hypothermia. Ultimately, when climbers fail on big mountains, it's usually not due to any one factor but rather to a multitude of them, including cold, dehydration, altitude, malnutrition, exhaustion, insomnia, and illness. The interaction of humans with the high mountains is very complex and, alas, still eludes our full understanding.
*Editor's note: John Grunsfeld returned to Denali in 2004 and successfully summited with three companions on June 7.
|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|